Barrett’s esophagus is a change in the lining of the esophagus caused by chronic reflux. Content from the stomach and small intestine flow back (reflux) into the esophagus and cause irritation. This irritation changes the lining of the esophagus and makes it similar to the lining of the stomach and the intestine.
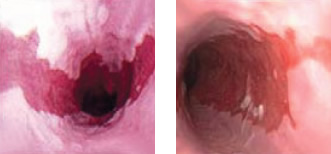
Endoscopic views of Barrett’s Esophagus
Symptoms
Barrett’s esophagus alone has no signs or symptoms. Because of its close connection with Gastroesophageal reflux disease (GERD), symptoms of GERD are often present and include:
Heartburn – A burning sensation that can run from your throat to the center of your chest
Regurgitation of sour liquid or food
Trouble swallowing (If you’re having trouble swallowing, seek care immediately)
Risk Factors
Based on these risk factors and your medical/family history, your doctor may recommend screening for Barrett’s esophagus.
Chronic Heartburn/Acid Reflux/GERD: Those who have chronic symptoms (more than five years) are more likely to develop Barrett’s esophagus.
Age: Barrett’s esophagus is more common in middle-aged and older adults. 55 is the average age of diagnosis.
Gender: Men are more likely to develop Barrett’s esophagus
Ethnic Background: White and Hispanic populations are at higher risk than other populations. Black and Asian populations have a lower risk of developing Barrett’s esophagus.
Smoking: Current and past smokers are more likely to develop Barrett’s esophagus.
Diagnosis
A doctor may suspect Barrett’s esophagus by reviewing a patient’s medical history, current symptoms, and risk factors. To confirm the diagnosis, doctors perform an endoscopy.
An upper endoscopy is a test that allows a physician to see the inside of the esophagus and stomach using a small lighted tube. After examining the appearance of the esophagus, the doctor may remove small tissue samples (biopsies) to make the diagnosis.
The diagnosis can be challenging due to anatomical differences in patients. Because Barrett’s esophagus doesn’t affect all the tissue in your esophagus, it can also be difficult to detect in some patients.
Three degrees of tissue change
Pathologists, doctors who are experts at examining tissue samples, will help confirm the presence of abnormal, precancerous cell growth (dysplasia) in your esophagus. Samples are often examined by two different pathologists. At least one of them should have special expertise in gastrointestinal disorders.
Pathologists will grade the dysplasia into one of three categories:
No dysplasia: Barrett’s esophagus is present, but precancerous changes are not found.
Low-grade dysplasia: Small changes in cells are present
High-grade dysplasia: Significant changes in cells are present. High-grade dysplasia is often the precursor to esophageal cancer.
Treatment
Treating Barrett’s esophagus depends on your overall health and extent of dysplasia in your esophagus.
Regardless of the dysplasia amount (if any), the primary goal of treating Barrett’s esophagus is to stop the damage to the esophagus. In most cases, this means eliminating acid reflux.
Foods that can worsen reflux include:
Acidic Juices like Orange and Tomato Juice
Coffee / Tea
Mint
Alcohol
Fatty foods
Behaviors that can increase acid reflux:
Eating right before bed
Lying down after eating
Eating very large meals
Lifestyle and Home Remedies to reduce acid reflux:
Maintain a healthy weight
Quit smoking
Raise the head of your bed: Place bricks or blocks under the head of your bed to elevate your head. About six inches is enough. This helps keep the acid in your stomach while you sleep.
Medications
Your doctor may prescribe medications that reduce the amount of acid in your stomach. These medicines are called proton pump inhibitors, or PPIs. Some of the more common PPIs include:
omeprazole (Prilosec, Zegerid)
lansoprazole (Prevacid)
pantoprazole (Protonix)
rabeprazole (AcipHex)
esomeprazole (Nexium)
dexlansoprazole (Dexilant)
Some of these medications, like omeprazole and lansoprazole, are available over-the-counter. You should discuss your signs and symptoms with a gastroenterologist if you have frequent heartburn or acid reflux.
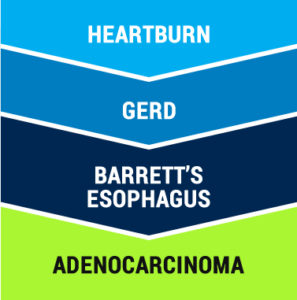
Complications
One potential complication of Barrett’s esophagus is that, over time, the abnormal esophageal lining can develop early precancerous changes. The early changes may progress to advanced precancerous changes, and finally to frank esophageal cancer. If undetected, this cancer can spread and invade the surrounding tissues.
However, progression to cancer is uncommon; studies that follow patients with Barrett’s esophagus reveal that only 0.5 percent of patients develop esophageal cancer per year. Furthermore, patients with Barrett’s esophagus appear to live just as long as people who are free of this condition. Patients often die of other causes before Barrett’s esophagus progresses to cancer.
Monitoring
For most people with Barrett’s esophagus, doctors recommend periodic screening endoscopies to look for signs of cancer. This approach is called surveillance. Your doctor will help you determine the best level of surveillance based on your condition.
Treatment – No Dysplasia:
Monitoring Endoscopy: Your doctor may recommend a monitoring endoscopy in one year, and then every 3 years after that if no abnormalities are found.
GERD Treatment: Controlling acid reflux is important. Lifestyle changes and medication can help reduce GERD symptoms. This is helpful when doctors try to locate and grade dysplasia.
Treatment – Low-Grade Dysplasia
Increased Medication: Those diagnosed with low-grade dysplasia are often asked to increase their dose of acid reducers (PPIs).
Monitoring Endoscopy: Doctors most often recommend another endoscopy within six months to look for any changes.
Endoscopic Resection – Endoscopic mucosal resection (EMR) uses an endoscope to remove dysplasia.
Treatment – High-Grade Dysplasia
High-grade dysplasia is often seen as a precursor to esophageal cancer. Because of that risk, your doctor may recommend the following treatments:
Endoscopic Resection – Endoscopic mucosal resection (EMR) uses an endoscope to remove dysplasia. EMR may be a reasonable alternative to esophagectomy in some patients.
Surgery/Esophagectomy – Complete removal of dysplasia, including all or part of the esophagus. The remaining part of your esophagus will be attached to your stomach. This type of surgery also carries the highest risk of complications, which should be considered carefully with your doctor. Your overall health, risk for cancer, and quality of life concerns should all be discussed beforehand.
Complications
Those with Barrett’s esophagus are at increased risk of developing esophageal cancer. The risk is very small, even among those with precancerous changes in the cells lining their esophagus. The vast majority of patients will not develop esophageal cancer.
FAQ
Is Barrett’s Disease the same thing as Barrett’s Esophagus?
Many people who search for Barrett’s disease are indeed referring to Barrett’s Esophagus.
To pay your bill online, please choose the correct option below: select the “Clinic Locations” button if you’re paying your Physician or Clinic Statement, or select the “ASC Locations” button if you’re paying your Procedure Statement at one of our Ambulatory Surgical Centers.
Gastroenterology Consultants of San Antonio (GCSA) is a Professional Association owned by the physicians that practice within it. GCSA’s physicians are directly involved in the management of patient services. GCSA physicians have indirect ownership interest in our Histology/Pathology, Anesthesia, Infusion and Ambulatory Surgical Centers (ASC).

 A doctor may suspect Barrett’s esophagus by reviewing a patient’s medical history, current symptoms, and risk factors. To confirm the diagnosis, doctors perform an endoscopy.
A doctor may suspect Barrett’s esophagus by reviewing a patient’s medical history, current symptoms, and risk factors. To confirm the diagnosis, doctors perform an endoscopy.